
ClickMedix, providing health services to underserved populations via mobile technology
The inclusive business initiative: providing affordable and quality health services to under-served populations by connecting patients to doctors through mobile technologies and community-based health providers to achieve continuous healthcare delivery to patients.
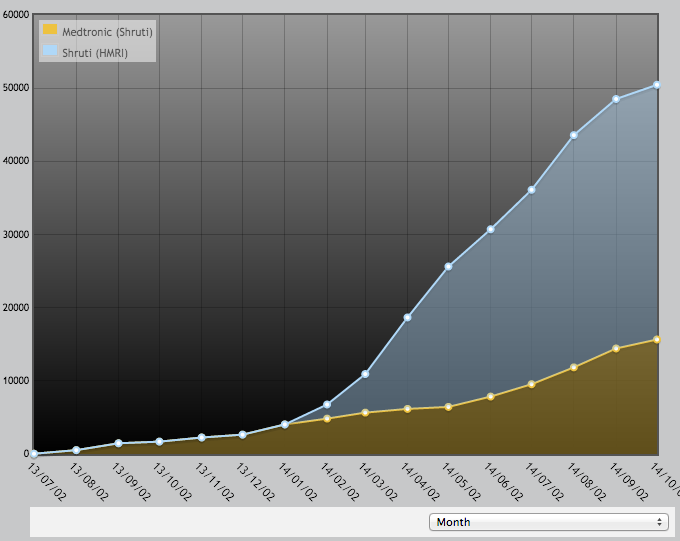
Social impact: reached more than 50,000 patients in India
Commercial stage: seeking series A investment
The idea for ClickMedix was conceived in 2008 during an MIT graduate school project. The company’s mHealth platform is now helping treat low-income people in more than ten countries. Founder and CEO, Ting Shih, shares the story of ClickMedix.
How did your inclusive business come into being?
My own background is in Computer Science and Six Sigma / Lean process improvement. I worked in the Department of Defense on weapons systems and then in GSK, and my strength is designing processes, or a ‘service chain’ that uses technology to add value.
Our initiative began as an MIT graduate school project. The question was how to effectively impact more than a billion people and address healthcare challenges in the developing world. The team did research to show that images could be used over a phone for medical diagnostics. This was 2008. At that time mhealth didn’t exist. This was a radical idea that needed to be proven.
We began our research pilot as a company called Click Diagnostics. That company dissolved and I started ClickMedix to commercialize the tele-consultation platform in late 2010.
One of the most significant changes in July 2013 was setting up a partnership with Medtronic (world’s large medical device firm that makes surgical instruments and provide surgical treatment for outpatient ear infections in addition to devices for heart disease and diabetes). They are partnering with us in India on a social business offering ear screening services and a path to affordable treatment and surgery for underserved patients.
What is the value proposition of your business?
ClickMedix is a healthcare technology company. We have developed a mobile health platform that connects health service providers, reduces cost of service delivery, and optimally utilizes tiers of existing health system for patient care. A community health-worker or a clinic nurse with a click-enabled mobile phone is able to act as the primary agent for service delivery, as she is connected to the mHealth platform and the entire health system along with medical specialists.
We have developed an application that translates clinical protocols into a series of questions on a phone and tablet or other mobile device, which a health worker can use to gather information and send relevant information to a remote expert on the platform. The patient interaction is done by a health worker (HW) who quickly learns the protocol by reading questionnaire prompts from the phone screen. They are linked to an expert doctor who reviews the images and information, and provides diagnosis.
Our goal is to find the best medical practice and scale it, and distribute it to where patients are. We are currently undertaking an ear screening initiative in India where low-income rural patients get free access to screening, the local health workers are able to administer basic treatment and refer patients to surgical facilities as needed through remote consultations by specialists that are displayed on the health worker’s phone.
ClickMedix operates in many other countries and covers a range of other issues. The largest population we’ve reached is in India where we are scaling fast. We have developed systems for diabetes and heart disease management, as well as podiatry screening, brain disease screening, and cancer screening systems.
How does your business work in practice?
The core of the business model is a user subscription fee for using the software that is paid by the health organizations who are screening and serving more patients through the use of ClickMedix. Our key principle is that the business model works for each person in the value chain:
- For doctors, they get new patients and a constant referral stream. Their job is to screen data that comes from each health worker and identify which patient conditions need procedural treatment, or provide instructions to enable health workers to administer treatment if possible.
- Our partner in India, Medtronic, set up the service chain with the hospitals, hiring the health workers that screen and refer patients using our software. The resulting increase in patients at their partner hospitals has been significant enough that the partner hospitals are now able to hire and fund their own community health workers to grow the program and reach more patients.
- The health workers tend to be young people around 17 to early 20’s, usually women. They receive training and income for their families, and they quickly acquire new skills because of the number of patients they see with similar problems. The data is used to compare the diagnosis of the doctor and the health worker and there is a 90 to 95% correlation.
- Patients get access to free health tests that were previously unavailable. Screening is currently free to patients, who later pay for treatment and medicines as usual. For example, they would pay for ear wax cleaning or antibiotics if there is an infection. These are provided at affordable rates.
Have partnerships been useful for your business?
Our main scaling strategy is partnerships particularly as we look to expand to retail pharmacy chains. Our technology is optimised for partnership. The partnership in India has led to rapid scale and has been successful for both companies. Medtronic wanted to explore if they could reach the BoP and their partnership with us increases their pipeline of patients from the BoP. Medtronic have developed an otoscope which attaches to an android phone that can be used by the health workers for patient screening.
The ear screening pilot took place in 2013 with five health workers in Delhi and Dr Shroff’s Charity Hospital. More than 10,000 patients have been screened here. In early 2014, we extended the model to Hyderabad where six health workers now see 1,000 patients per week.
Medtronic screening is likely to cover 10 times as many patients in the coming year as the past year.
What stage of financing are you at?
We have been self funded so far although we have won over $100,000 in grants and awards. We are currently looking for Series A range investment but have not been active in pitching.
What commercial success have you seen so far?
We reached breakeven at the end of 2013. A big challenge has been learning about the economics of the healthcare system, which is immensely complicated. The main challenge now is setting pricing policy. If the pricing is wrong it can take 10 to 20 years to get a proper return ready for an IPO. Currently, charges are $5-$25 per health worker to Medtronic and $50 – 200 per user (nurse or doctor) in the United States. There are different pricing models and getting it right is hard at this pace of scale. The investor community thinks I’m undercharging!
We are targeting a turnover of $100 million in 5 year’s time.
What social impact are you having?
In India, the Medtronic ear screening has reached more than 50,000 people in one year, resulting in over 1,500 patients being treated at affordable rates. The programme will reach ten times as many in the coming year. Ear screening in India is otherwise totally neglected.
In other countries, we have few clinics so far but will reach more than 10,000 per clinic over time.
We measure our impact by looking at the data we collect through the software platform. We are also able to track treatments provided overtime and explore improved treatment regimens as well as effective screening and triage protocols over a growing population.
What key lessons have you learnt in your inclusive business journey so far?
The main lesson has been learning to follow the money and understanding the stakeholders that we touch. It took five years to understand the money flow of health systems. Patients don’t typically pay for healthcare. It’s the government, charity, or private company that pays from its pocket. There are multiple players involved.
You have to follow the money for each stakeholder. Work out who cares, who currently pays, why would they pay for our service – how would it affect their bottom line by lowering their costs or increasing their revenue.
We’ve learnt that healthcare marketing is done very differently. Deciphering the marketing message and being able to describe it in a right way has taken many years.
In this series, we speak to some of the ‘Breakthrough SMEs’ identified in the Business Call to Action’s (BCtA) Flagship report Breaking Through: Inclusive Business and the Business Call to Action Today. These are all small and medium enterprises that are emerging as influential actors in inclusive business. These interviews will uncover the stories of these SMEs – what sets them apart from other businesses, how are they overcoming the many challenges at the BoP and what factors are driving their success?